Immunochemotherapy versus rituximab in anti-MAG neuropathy: a report of 64 patients
Résumé
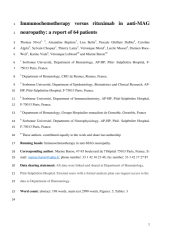
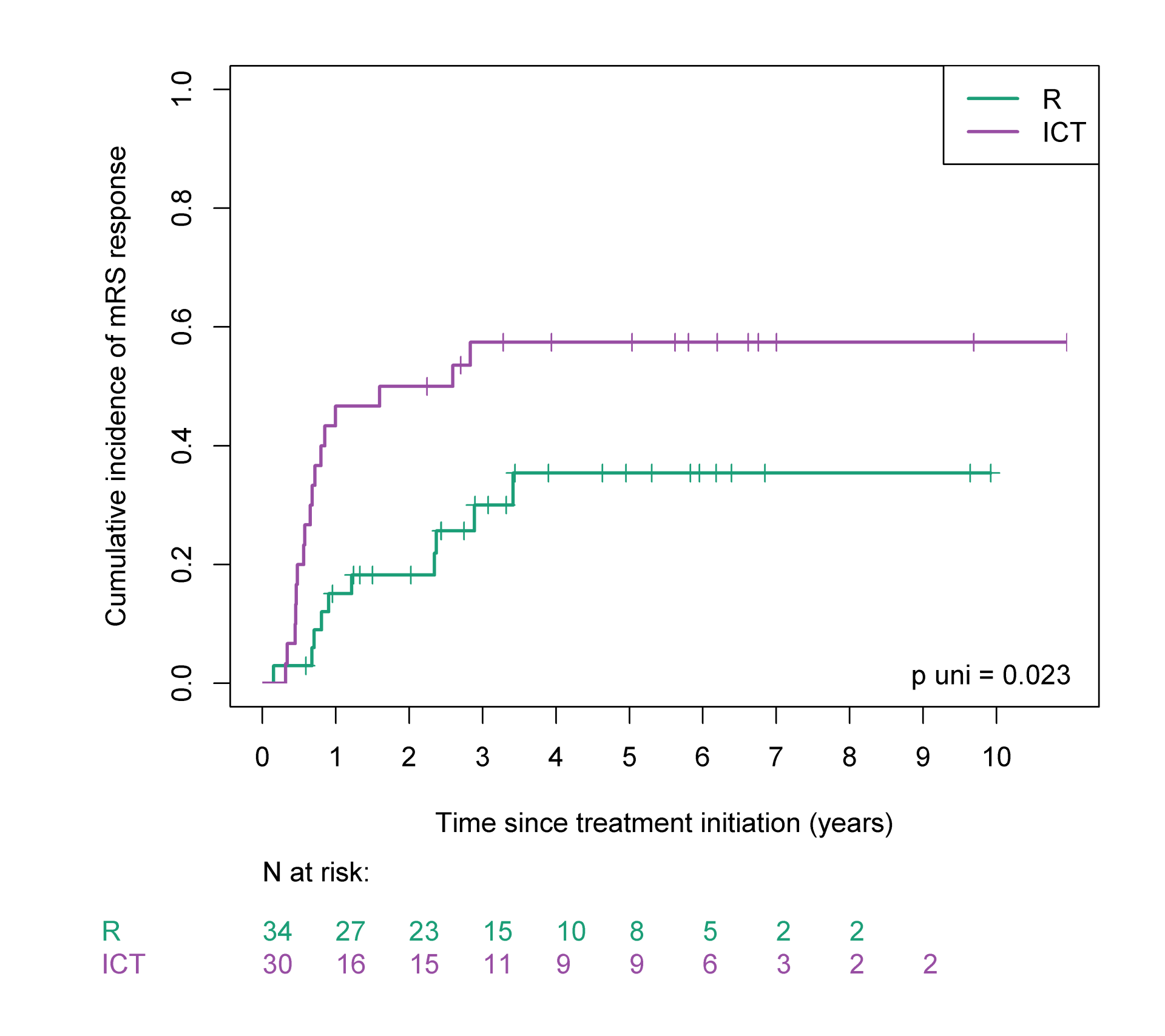
Monoclonal immunoglobulin M (IgM) anti-myelin-associated glycoprotein (MAG) neuropathy is a rare disabling condition, most commonly treated with rituximab monotherapy (R), which leads to neurological improvement in only 30%-50% of patients. The combination of rituximab plus chemotherapy has been proven to improve the level of responses. We studied the outcomes of anti-MAG neuropathy patients treated either by R, or by immunochemotherapy (ICT) in our centre, focusing on the incidence of the first neurological response evaluated by the modified Rankin Scale (mRS). From 2011 to 2018, 64 patients were studied: 34 were treated with R and 30 with ICT. According to our treatment decisionmaking process, the median mRS was higher in the ICT group (mRS 2) compared to the R group (mRS 1). At 1 year, mRS improvement rates were 46% and 18% of the ICT and R groups of patients respectively, with a median time to response of 8 and 13 months (p=0.023). Adverse effects were higher in the ICT group: 62% vs 15% (p˂0.01) all grades included. One secondary acute leukaemia occurred 5 years after treatment by ICT. In conclusion, ICT may be used as a valid option for patients with rapidly progressive and/or severe anti-MAG neuropathy symptoms.
Fichier principal
 baron_ms cleaned version V2.pdf (415.45 Ko)
Télécharger le fichier
Fig.1_mRS_response.png (107.04 Ko)
Télécharger le fichier
Fig.2 Mean mRS.png (138.49 Ko)
Télécharger le fichier
Fig.3 Time to new treatment.png (119.79 Ko)
Télécharger le fichier
Fig.4 Individual profiles.png (588.77 Ko)
Télécharger le fichier
Fig.5 Concordance.png (195.85 Ko)
Télécharger le fichier
baron_ms cleaned version V2.pdf (415.45 Ko)
Télécharger le fichier
Fig.1_mRS_response.png (107.04 Ko)
Télécharger le fichier
Fig.2 Mean mRS.png (138.49 Ko)
Télécharger le fichier
Fig.3 Time to new treatment.png (119.79 Ko)
Télécharger le fichier
Fig.4 Individual profiles.png (588.77 Ko)
Télécharger le fichier
Fig.5 Concordance.png (195.85 Ko)
Télécharger le fichier
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Origine | Fichiers produits par l'(les) auteur(s) |
|---|
| Origine | Fichiers produits par l'(les) auteur(s) |
|---|